
Darker red areas represent counties that have more "deaths per 100k people".
|
Cultural HistoryAs we understand that the term "strange fruit" refers to the lynched human bodies hanging in trees for public entertainment, you see that racism had a very dehumanized stigma attached to it. Unfortunately, research and studies show that "racist violence committed in the past has health implications today" (Haskins). According to co-author Sandra Glover, “the root cause that drove the lynchings in that period still is in place today…so dealing with the root causes of health disparities is dealing with racism". (Haskins).
Counties where lynchings were took place had higher proportions of black residents as well as higher average unemployment and wealth disparities among households. In counties without lynchings, there was a higher proportion of adults lacking health insurance. Among white populations, living in a county with historic lynchings was associated with higher mortality rates — a finding that suggests racist violence has negative impacts across racial groups, according to researchers. the Director of South Carolina's Health Research Center told reporters that “it may be that people are adversely affecting the social determinants of health for all when they are disenfranchising minority populations" (Haskins). Whatever the cause may be, the notion still holds that racism plays a significant role in access to healthcare and the medical resources such as primary health doctors, health insurance, urgent care acceptance, etc. |
How does racism affect health? Health inequities are seen in many outcomes, including infant mortality, heart disease, and cancer. A century ago, W.E.B. Du Bois recognized the connection between societal inequities and health inequities, raising several central arguments related to racism, poverty, and other social problems. He noted, “The Negro death rate and sickness are largely matters of [social and economic] condition and not due to racial traits and tendencies” (Gee and Ford)
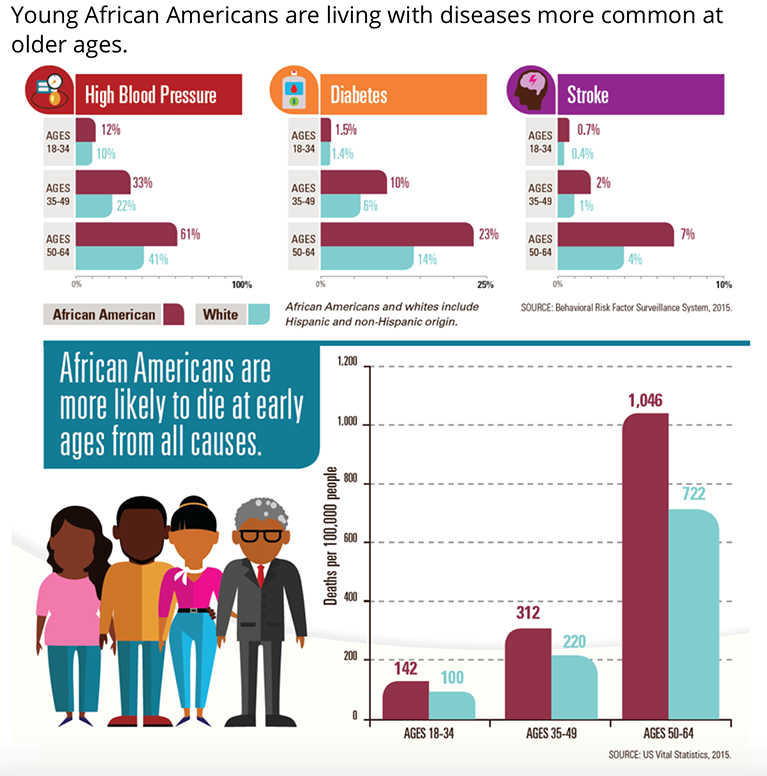
In the U.S., health disparities between blacks and whites run deep. For example, blacks have higher rates of diabetes, hypertension, and heart disease than other groups, and black children have a 500% higher death rate from asthma compared with white children. Williams and Lavizzio-Moruey write that geography plays a large role in all of this because, “where we live determines opportunities to access high-quality education, employment, housing, fresh foods or outdoor space – all contributors to our health.”On average, white Americans spent 80 minutes waiting for or receiving care, while black Americans spent 99 minutes and Latinos 105 minutes waiting for that same care. "These inequalities contribute to gaps in health insurance coverage, uneven access to services, and poorer health outcomes among certain populations. African Americans bear the brunt of these health care challenges" (Taylor). |
|
|
|
Does where you live matter?In the largely black East Lake district in Atlanta, Purpose Built Communities is breaking the cycle of poverty by addressing housing, education, crime, jobs and other factors that impact health simultaneously.There is no single solution for the confluence of societal racism, poverty and other factors that lead to poor health. However, we now know enough to improve the situation. Health builds from where we live, learn, work and play – and only secondarily in the doctor's office. "Data conclusively show that early childhood education matters greatly, as does the nutritional value of the food we put in our bodies and our access to safe outdoor spaces. We need to work on all those and other social and economic fronts in underserved communities" (Williams). But we also need to acknowledge the connection between racism and poor health and actively work to close that gap so that everyone has the best opportunity for good health. As Martin Luther King Jr. is often attributed as saying, "Of all the forms of inequality, injustice in health is the most shocking and inhumane."
|
F A C T S A B O U T H E A L T H C A R E D I S P A R I T I E S
1.Because African Americans tend to be poorer than other demographic groups on average, public health insurance programs such as Medicaid are vital to ensure affordable health care and healthier outcomes—yet fourteen states have resisted Medicaid expansion, mostly in the South.
5.Nearly half (46 percent) of nonelderly black adults who do not have insurance report having one or more chronic health conditions. (Russell)
|
2.Certain social determinants of health, such as poverty, income inequality, wealth inequality, food insecurity, and the lack of safe, affordable housing have important implications for health risk and the ability to attain health insurance coverage for African Americans
6.African Americans, American Indians/Alaska Natives and multi-race populations had a higher rate of cigarette smoking in 2015 than other race/ethnic groups. (Pèrez)
|
3.Compared with metro areas, non-metro areas have a higher age-adjusted death rate and a greater percentage of potentially excess deaths from the five leading causes of death (Pèrez)
7.Significant disparities exist in medical education; of all medical school graduates in 2014, only six percent were African American, five percent were Latino and less than one percent were American Indian or Alaska Native. (Pèrez)
|
4.“Socio-economic status matters”; lower income households are three times more likely to die “from anything” than households earning more than $115,000. (Pèrez)
8.Adult obesity rates for African Americans are higher than those for whites in nearly every state of the nation—37 percent of men and nearly 50 percent of women are obese.(Russell)
|
